
Anterior cruciate ligament injuries in children and adolescents
What does a child’s ACL look like?
The ACL in a child passes from the shin bone (tibia) to the thigh bone (femur), similar to an adult’s ACL but in a slightly more horizontal direction. Also just above and below the insertions of the ACL into the bones, there are growth plates.

Paediatric ACL from the front
How is the child’s ACL injured?
The ACL is commonly injured during pivoting sports such as soccer, skiing, racket sports.
The most common type of injury is a noncontact twisting injury with the foot planted on the ground. Other injuries can include hyper extension or a direct contact to the shinbone.
How do I know if my kid has torn their ACL?
Most often during sports or activities they have had a noncontact twisting injury where they feel or hear a snap. They often fall to the ground and the knee swells up immediately and is painful. They are generally unable to continue doing the activity they were doing or playing the sport they were playing.
If it is several months or even years after their original knee injury, the swelling may have resolved, but if they are feeling that they can’t “trust the knee” or if it is collapsing or giving way when turning or pivoting and feeling unstable, one of the causes of this may be an undiagnosed ACL tear.
There are times when the ACL ruptures with less pain and swelling.
What’s the difference between an ACL tear, rupture or injury?
There is no difference between ACL tear, rupture or injury. The terms are interchangeable.
Why are kids ACL injuries becoming more common?
ACL injuries in children are becoming increasingly common. Although the cause of this is not confirmed, it is likely that children are playing more competitive sports more frequently, many adolescents are also much bigger in height and frame than they were 20 years ago, and injuries are being diagnosed more frequently because MRI scans are readily available.
What is the mechanism of paediatric ACL injury?
Most paediatric anterior cruciate ligament injuries occur as the result of a noncontact twisting injury. This can occur in twisting sports such as soccer, netball, skiing, lacrosse, basketball.
As with adults, the shin bone moves out of position relative to the thigh bone, the so-called pivot type injury.
Can other structures be injured as well as the ACL?
The most common structures that are involved that are injured in conjunction with the ACL are the medial collateral ligament, meniscal cartilages, and sometimes bruising occurs on the bones of the femur and tibia, the so-called pivot bone bruise or impaction fracture.
How do we diagnose paediatric ACL injuries?
As with adults, diagnosis depends on a thorough history of the accident, and examination of the knee, particularly when it is less sore or swollen.
Is an MRI scan necessary to diagnose an ACL injury?
It is becoming increasingly clear that any child who has a swollen knee as the result of an injury should have an MRI scan to determine which structure has been damaged. ACL injuries are most commonly confirmed by MRI scanning.
What does a kid’s ACL injury look like on MRI scan?
Reading MRI scans is a complex process.
The scan effectively slices the knee in three different directions. We look for differences in greyness in the structures. This is known as signal. A white or light grey area is known as high signal (on “fat saturated”images).
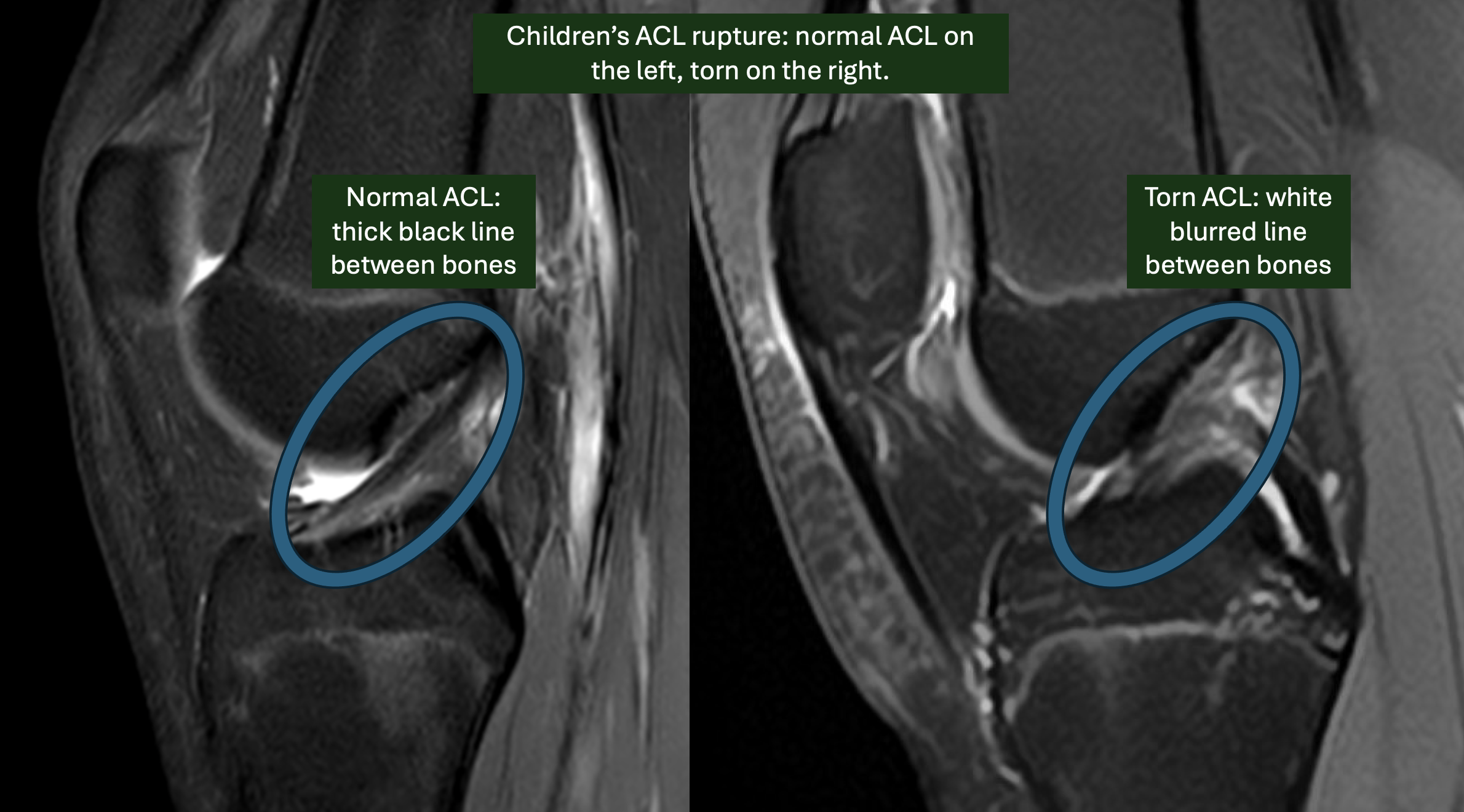
ACL injuries show high signal in the substance of the ACL or where the ACL attaches to the femur or tibia.
Can children's ACL injuries be managed without surgery?
Whilst it is possible to manage paediatric ACL injuries without surgery, long-term studies have shown better results with ACL reconstruction. In particular, reconstruction of the ACL leads to a more stable knee and prevent further damage to the meniscal cartilages.
The British knee Society, therefore recommends that all paediatric anterior cruciate ligament injuries are treated by a surgeon that is appropriately qualified and experienced in management. Early surgery and reconstruction should be considered.
What does a paediatric ACL reconstruction involve?
The operation involves taking tendon from another part of the knee and transplanting this where the damaged cruciate ligament is situated in order to replace this ligament. This is known as autograft anterior cruciate ligament reconstruction.
Which donor site can be used?
The most commonly used tendon is the hamstring tendon on the inner aspect of the thigh and knee. These tendons are the gracilis and semitendinosus tendons. Other tendon grafts include the quadriceps tendon.

Graft choices for ACL reconstruction
If the teenager is fully grown with no growth left, patella tendon can be used.
How do you replace the damaged ACL?
There are many different techniques to plug the new graft into the bone.
Most commonly, tunnels are drilled in the shin bone and the thigh bone. The graft is then passed through the tunnels. This is known as the transphyseal technique and is often used in patients over the age of 12 or 13 by many paediatric ACL surgeons.

ACL reconstruction
The graft then may be fixed in the thigh bone and the shin bone with some form of suspensory button or Screw fixation.

Paediatric ACL reconstruction. These front and side Xray pictures are taken during the operation to ensure good tunnel and suspensory button positions that are not interfering with the growth plates..
Which are the different techniques for paediatric ACL reconstruction?
There are many different techniques as illustrated below. All of these have pros and cons. Essentially, they try to address the following considerations:
give a stable knee for pivoting sports and impact.
minimise the risk of growth disturbance
give a strong graft with a low risk of rerupture
minimise long term pain or weakness from the donor site
In summary of the literature from research:
donor allografts have a high risk of rerupture and are not generally advised for paediatric ACL reconstruction
patellar tendon/bone grafts can only be used in the fully mature skeleton
hamstring grafts are the most commonly used in the skeletally immature adolescent in most countries
quadriceps tendon is showing promising results but needs further long term data.

Paediatric ACL Reconstruction operation techniques
What is the risk of growth disturbance?
The risk of growth disturbance is low, between 0.5-1%. It is not clear whether growth disturbance is caused by damage to the growth plates or by tethering of the graft that affects growth. There are techniques that do not breach the growth plates, but there is debate amongst paediatric ACL surgeons as to when they should be utilised and whether they do indeed reduce the risk of growth disturbance. Mr Gupte considers many factors when employing a particular technique. Some of these techniques are illustrated below.
What is a lateral tenodesis reinforcement and why might it be used?
A lateral tenodesis is a modification of a very old ACL reconstruction technique know as the “Macintosh technique”. Mr Gupte was involved in the research team at Imperial College London that helped in the development of this technique from 2010. The technique involves taking a piece of tissue on that ins already present in the outside (lateral side) of the knee called the iliotibial band. A strip of this tissue is passed underneath the lateral collateral ligament and tethered to the thigh bone (femur) on the outside of the knee: proximal and posterior to the lateral epicondyle.
The biomechanics studies that took place at Imperial and other centres suggested that this technique reduces the stress on the ACL graft especially in the pivoting phase of movement such as during sharp turns and decelerating movements in sport.
Although not all surgeons employ the lateral tenodesis reinforcement technique, several studies have shown a lower re-rupture rate of ACL graft after return to sports in certain patient groups after lateral tenodesis.
Mr Gupte utilises the “modified Lemaire” technique of lateral tenodesis.

Lateral tenodesis operation to “reinforce” ACL graft: modified Lemaire technique
When is lateral tenodesis used for ACL surgery?
Mr Gupte discusses whether lateral tenodesis may be indicated with patients and their relatives. In general lateral tenodesis is used in cases of:
hypermobility
excessive knee hyperextension
most paediatric cases
revision knee ACL reconstruction
What does a lateral tenodesis scar look like?

Lateral tenodesis scar in left knee. Please note: scars vary in size and thickness and colour depending on individual patient requirements, skin colour and genetics.
How do you decide which type of ACL reconstruction in child?
There are many factors that decide this:
Age and skeletal maturity. Below the age of 11 years it is best not to disturb the growth plates of the bone and there are certain techniques that are used known as extra physeal ACL reconstruction.
Between 11 and 14 years, different surgeons use different techniques. Mr Gupté uses a trans-physeal, (physeal respecting) technique involving minimal damage to the growth plates and several precautions being taken to avoid growth plate injury.
Between the ages of 15 and 18 in girls and 16 and 18 in boys, an adult type ACL reconstruction can be considered if the growth plates are determined to be fully closed.
What is ACL repair and does it work in a child?
ACL repair, where the torn ACL is stitched back into the femur/thigh bone, sounds like a very good idea. Using the body’s own torn ACL tissue rather than new ACL graft from somewhere else. It has been tried in various forms for the last 40 years. Unfortunately most research series have shown a much higher re-rupture rate for ACL repair (up to 40%) than reconstruction. Whilst there may be some promising new techniques in ACL repair, the British guidelines are that ACL repair should only be performed as part of a clinical trial given its poor track record. Such trails will take place soon. Mr Gupte does not think the evidence is strong enough to offer ACL repair to his patients at the moment.
What happens after ACL surgery?
Most commonly needs placed in a brace and crutches are required for between four and six weeks after surgery. We then follow a five stage rehabilitation protocol as detailed in the attached PDF in the patient resources section of this website.
What is the success and rerupture rate after ACL reconstruction?
This really depends on the nature and age of the injury as well as whether the patient has hyperlax or elastic joints.
The quoted failure rate of ACL reconstruction in under 18s is between seven and 15% at five years.
This does however mean that 85-93% of children will have a good result with a stable knee that allows a return to sport.
The failure rate is likely to be higher in children than adults because children have an inherent elasticity to their tendons which make them more prone to be rupture.
In children and adolescents, bone growth probably leads to more stress on the newly transplanted tendon and this can predispose to rupture later on.
Most knee surgeons will also recommend a slower rehab protocol for children than adults, as the rerupture rate is higher if children return to full sports before 10-12 months
There are many techniques thought to improve success rate after ACL reconstruction children.
These include:
Using a thicker tendon graft
fixing the graft on the bone with more secure methods.
Performing a supplementary operation known as a lateral extra-articular tenodesis. This effectively gives a second anterior cruciate reinforcement on the outside of the knee. Although this does involve an extra scar biomechanical studies show that these knees are probably stronger especially in hyper lax patients.
The best knee surgeons in children’s and adolescent knee surgery will take into account the needs of the individual child, the nature of the injury, the biology of the knee and the child's body, and psychology. They will thn employ the most biomechanically sound techniques with a good evidence base that minimises the risk of complications and maximises the chances of a successful result.
Relevant PDF documents (downloads):
Anterior cruciate ligament injuries in children and adolescence
Pediatric ACL Injuries: A Review of Current Concepts